Introduction
DSM study mistakes are one of the biggest reasons psychology students struggle with the DSM-5-TR.
Many students spend hours reading diagnostic criteria, highlighting pages, and creating flashcards. Yet when they’re asked to discuss a clinical case, compare two similar disorders, or explain a differential diagnosis, things suddenly become much less clear.
The issue is often not motivation.
The issue is method.
The DSM-5-TR is one of the most important resources used in psychology, counseling, social work, and mental health training. At the same time, it’s one of the most misunderstood study tools.
Students frequently approach it as if it were a traditional textbook. In reality, the DSM serves a very different purpose.
If you’re still getting familiar with the structure of the manual, start with our guide:
A Beginner’s Roadmap to the DSM-5-TR
In this article, we’ll look at five common DSM study mistakes and explore more effective alternatives.
Mistake #1: Reading the DSM Like a Traditional Textbook
Many students open the DSM-5-TR and start reading from the beginning.
At first, this feels productive. You’re studying. You’re making progress. You’re covering material.
The problem appears a few weeks later.
After reading dozens or even hundreds of pages, much of the information begins to blend together. Diagnostic criteria start to feel repetitive. Categories become difficult to remember. Motivation drops.
The reason is simple.
The DSM was never designed to function as a teaching textbook.
It is primarily a classification and diagnostic reference system.
Most clinicians don’t learn diagnosis by reading the manual from cover to cover. They learn by combining foundational knowledge, clinical examples, supervision, and repeated exposure to symptom patterns.
A Better Approach
Instead of trying to read everything, focus on understanding:
- The major DSM categories
- How disorders are grouped
- The logic behind diagnostic classification
- Relationships between similar disorders
Think of the DSM as a map rather than a novel.
You don’t memorize every road before taking a trip.
You learn how the map is organized and then use it when needed.
Mistake #2: Memorizing Criteria Without Understanding Symptom Patterns
Students often believe that success comes from memorizing every criterion exactly as written.
While criteria matter, memorization alone rarely produces clinical confidence.
Consider two students:
The first can recite diagnostic criteria word for word.
The second can explain how a disorder typically presents, what symptoms tend to cluster together, and how the condition affects daily functioning.
Which student is closer to thinking like a clinician?
Usually the second.
Experienced professionals often recognize patterns before they mentally review diagnostic criteria.
They notice timelines.
They notice symptom clusters.
They notice functional impairment.
They notice what doesn’t fit.
A Better Approach
When studying a diagnosis, ask yourself:
- What does this disorder typically look like?
- What symptoms tend to appear together?
- What would this look like in a real person?
- What makes this presentation distinctive?
The goal is not simply to remember information.
The goal is to recognize meaningful patterns.
Mistake #3: Studying Disorders One at a Time
This mistake is surprisingly common.
A student spends one week studying Generalized Anxiety Disorder.
The following week, they study Panic Disorder.
Then Social Anxiety Disorder.
Each diagnosis is treated as an isolated topic.
Unfortunately, patients don’t present themselves in isolated chapters.
Many DSM disorders share overlapping symptoms.
Anxiety disorders are a perfect example.
Someone experiencing excessive worry, physical tension, avoidance, sleep difficulties, and concentration problems may fit multiple diagnostic possibilities.
This is why studying disorders separately often creates confusion rather than clarity.
A Better Approach
Study related disorders together.
Compare them side by side.
Examples include:
- Major Depressive Disorder vs Persistent Depressive Disorder
- OCD vs Generalized Anxiety Disorder
- Social Anxiety Disorder vs Avoidant Personality Disorder
- Bipolar Disorder vs Major Depressive Disorder
The contrasts often teach more than the diagnoses themselves.
Students frequently report that differences become obvious only when disorders are directly compared.
Mistake #4: Ignoring Differential Diagnosis Until the Last Minute
Many students spend months learning diagnostic criteria before paying serious attention to differential diagnosis.
This creates a problem.
Differential diagnosis is where much of the real learning happens.
Knowing that a person meets criteria for a disorder is useful.
Understanding why alternative diagnoses do not fit is often more valuable.
Consider the difference between these questions:
“What is OCD?”
versus
“Why is this OCD and not Generalized Anxiety Disorder?”
The second question requires deeper reasoning.
It forces you to evaluate similarities, differences, exclusions, and clinical judgment.
This is the point where many students begin transitioning from memorization toward genuine diagnostic thinking.
A Better Approach
Whenever you study a diagnosis, create a short comparison list:
- Disorders that look similar
- Key overlapping symptoms
- Features that distinguish them
- Common diagnostic errors
If you’d like a practical framework for approaching the DSM more efficiently, you may also find helpful:
How to Study the DSM-5-TR Without Reading It Cover to Cover
Mistake #5: Delaying Clinical Application
A common belief among students is:
“I’ll start working with cases once I know the DSM better.”
The problem is that clinical reasoning develops through application, not through passive reading alone.
Imagine learning to drive by reading manuals for six months without ever sitting behind the wheel.
Knowledge matters.
Practice matters too.
The sooner you begin applying concepts to clinical scenarios, the faster your understanding improves.
You don’t need to wait until you’ve mastered the DSM.
Very few professionals would claim they have memorized every section of the manual.
A Better Approach
After studying a disorder:
- Read a brief case vignette
- Identify possible diagnoses
- Justify your reasoning
- Consider alternative explanations
- Review the differential diagnosis
Even simple exercises can dramatically improve retention and understanding.
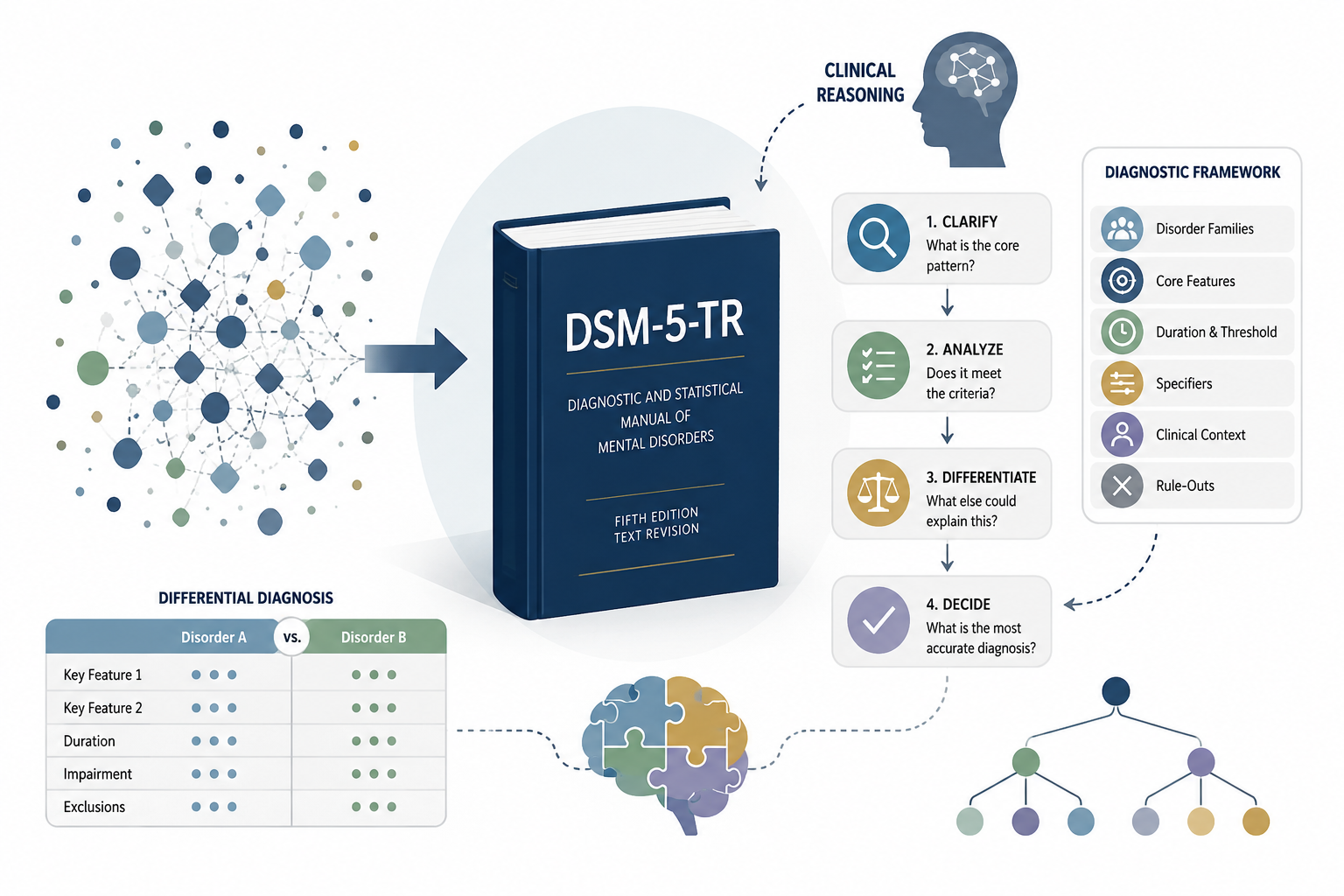
The Shift That Changes Everything
Most students begin by asking:
“What diagnosis is this?”
More experienced clinicians often ask:
“What information helps me distinguish between the most likely possibilities?”
That shift changes the entire learning process.
Instead of collecting isolated facts, you begin organizing information into meaningful diagnostic frameworks.
The DSM starts feeling less like a massive collection of criteria and more like a system you can actually navigate.
This is often the point where studying becomes faster, more structured, and considerably less frustrating.
Looking for a More Visual Way to Study the DSM?
Many students learn best when information is organized visually.
Comparison tables, symptom maps, diagnostic summaries, and differential diagnosis charts can make complex material easier to understand and remember.
That’s exactly why we created the DSM-5-TR Visual Guide.
Rather than replacing the DSM, it was designed to help students and trainees organize information more efficiently, identify key distinctions between disorders, and strengthen clinical reasoning skills.
Our DSM-5-TR Visual Guide is available on Amazon.
Conclusion
Most DSM study mistakes have little to do with intelligence or effort.
They stem from using strategies that prioritize memorization over understanding.
Students who focus on symptom patterns, differential diagnosis, clinical application, and diagnostic comparisons often develop confidence much faster than those who try to memorize every page.
The DSM is an essential resource.
But the ultimate goal isn’t to memorize the manual.
The goal is to learn how to think with it.
Great content! Keep up the good work!
Your writing has a way of resonating with me on a deep level. I appreciate the honesty and authenticity you bring to every post. Thank you for sharing your journey with us.
helloI really like your writing so a lot share we keep up a correspondence extra approximately your post on AOL I need an expert in this house to unravel my problem May be that is you Taking a look ahead to see you