Introduction
You sit down with the DSM-5-TR, open a disorder you are supposed to know, and the same thing happens again: the page looks clear until you try to use it. The criteria seem understandable while you read them. Then a case vignette appears, two disorders look similar, and your confidence drops. That gap is the real problem.
Many psychology students assume the DSM becomes easier once they spend enough hours reading it. In practice, the opposite often happens. The more criteria you read without a system, the more the disorders start blending together. The DSM-5-TR is a reference manual, not a learning system. If you study it like a textbook, it will punish you with detail before it gives you structure.
Common mistake: you try to fix confusion by reading more pages. You highlight criteria, reread the same section, and hope the wording will become familiar enough to stay. Familiarity does improve, but usable knowledge often does not. A week later you may recognize the paragraph and still be unable to explain why one diagnosis fits better than another.
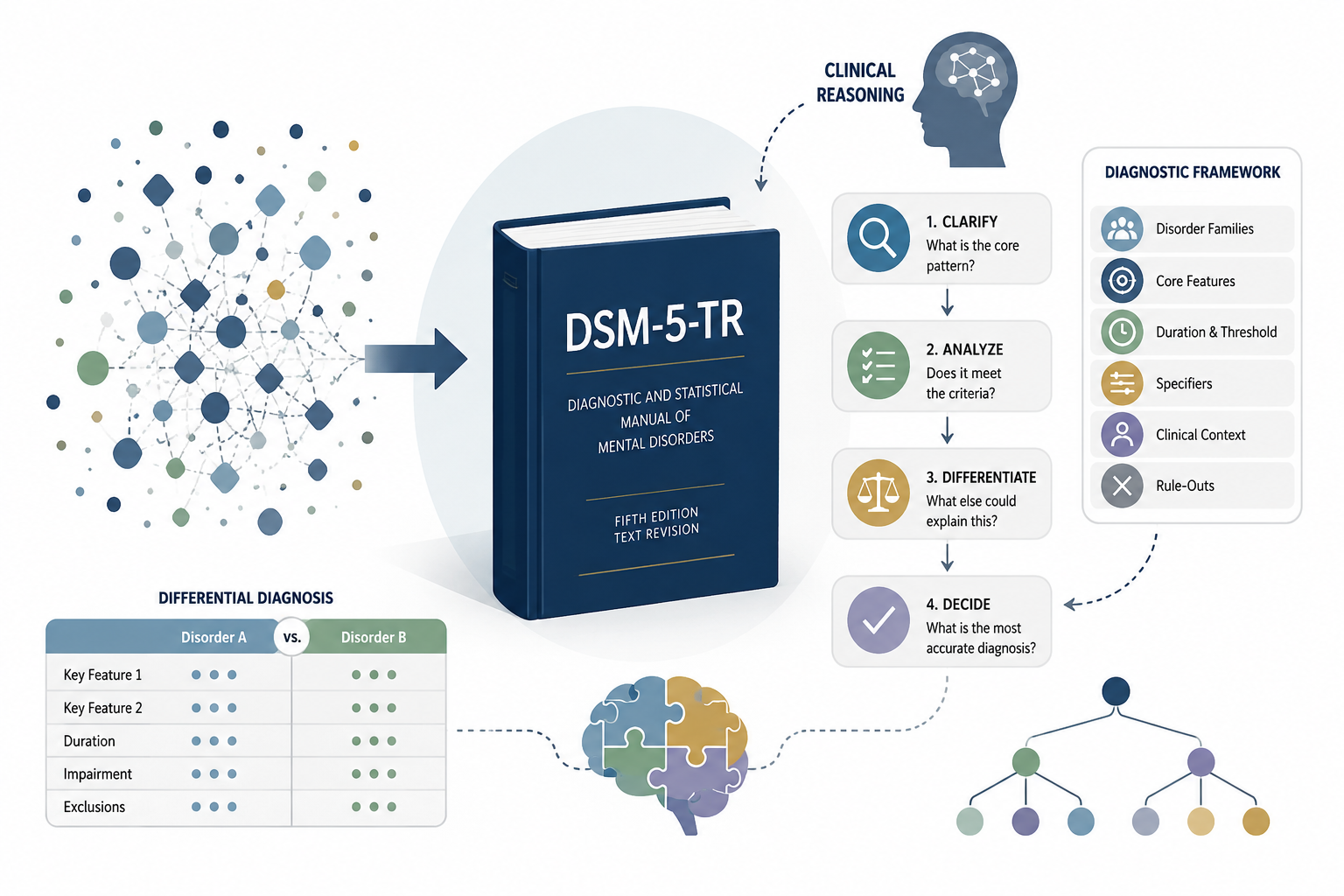
What works better is to study the DSM as a set of clinical decisions. Before you memorize a criterion, ask what it helps you decide. Does it set a threshold? Separate one disorder from another? Rule something out? Describe severity or course? That question is the heart of a beginner’s roadmap to the dsm-5-tr.
Practical takeaway: before you study any disorder, write one sentence that starts with: “The diagnostic decision here is…” For major depressive disorder, that decision is not just “is the person sad?” It is whether a specific depressive episode pattern is present, whether it reaches threshold, and whether another explanation changes the diagnosis.
Stop reading it cover to cover
Reading the DSM-5-TR cover to cover feels responsible. It also feels safe. If you are anxious about missing something, moving page by page gives you the sense that you are doing the serious version of studying. The problem is that passive coverage does not create clinical reasoning. Exposure is not the same as understanding.
What usually happens is predictable. You start with one disorder, underline several phrases, move to the next disorder, and keep going. By the end, you have seen a lot of information but have made very few decisions. Your mind has not been forced to ask what separates one presentation from another, so the material remains flat.
Mini case: imagine a vignette about low mood, poor sleep, low energy, guilt, and difficulty concentrating. If you only read the depressive disorders chapter, you may reach for major depressive disorder too quickly. But a better diagnostic habit makes you pause: was there any past hypomania? Is this grief? Is there substance use? Is the duration enough? Is impairment clear? Differential diagnosis starts where memorization stops.
What works better is targeted reading. Before you open the manual, give the reading a job:
- What is the core pattern?
- What must be present?
- What changes the diagnosis?
- What rules it out?
- What commonly gets confused with it?
That list turns reading into clinical sorting. You are no longer trying to absorb everything. You are learning what each detail does.
If you’re looking for a more detailed study strategy, you may also find our guide on how to study the DSM-5-TR without reading it cover to cover helpful.
Build a diagnostic map before you memorize details
One pattern shows up again and again: you try to memorize criteria before you know the shape of the disorder family. That is like memorizing street names before you know the city map. You may remember pieces, but you do not know where they belong.
A diagnostic map gives the details a home. Start with four layers:
- the disorder family
- the core pattern
- the threshold or duration rule
- the closest rule-outs
This is not extra work. It is the work that makes the criteria usable. Every criterion is easier to remember when you know the decision it supports.
Example: panic disorder is not simply “panic attacks.” Panic attacks can appear in many clinical pictures. The useful distinction is recurrent unexpected panic attacks followed by persistent concern or behavioral change. If you miss that pattern, you may confuse panic disorder with social anxiety disorder, PTSD, specific phobia, substance-related panic, or panic attacks occurring inside another disorder.
Practical lesson: when a symptom appears in many disorders, do not study it as a standalone fact. Study the pattern around it. Panic attacks are not enough. Low mood is not enough. Intrusive thoughts are not enough. The diagnosis depends on the pattern, threshold, context, and rule-outs.
Turn criteria into clinical questions
A criterion becomes easier to remember when it becomes a question you could actually use. This is where many students get stuck: they try to memorize DSM language without translating it into assessment language. The result is wording that feels familiar but does not guide the interview or the case formulation.
Try this conversion:
- Duration rule: “How long has this been happening?”
- Impairment rule: “What changed in daily functioning?”
- Exclusion rule: “What else could explain this?”
- Specifier: “What kind of presentation is this?”
This shift matters because clinical assessment is built from questions, not memorized sentences.
Scenario: you are studying generalized anxiety disorder. The criterion about excessive anxiety and worry is not useful until you ask what the worry attaches to, whether it is difficult to control, what physical or cognitive symptoms appear with it, and whether another disorder explains the pattern better. Without those questions, GAD becomes a vague label for “a lot of worry.”
Common mistake: you ask whether the symptom is present, then stop. What works better is to ask what the symptom means diagnostically. Concentration problems can appear in depression, anxiety, ADHD, trauma-related presentations, sleep problems, substance use, and more. The useful question is not only “is concentration poor?” It is “what pattern makes concentration poor here?”
Use comparison to make differential diagnosis easier
Differential diagnosis is usually the moment when memorization stops feeling impressive. Two disorders can share sleep problems, concentration difficulty, irritability, avoidance, low mood, or intrusive thoughts. If you study only symptom lists, overlap feels like a threat. If you study diagnostic decisions, overlap becomes manageable.
The common mistake is comparing disorders too late. You first memorize them separately, then try to compare them during an exam or case discussion. That is backwards. Comparison should be part of learning, not a final review activity.
Example: OCD and generalized anxiety disorder can both involve repetitive mental activity. The useful distinction is not a tidy vocabulary contrast between “obsession” and “worry.” You need to ask whether the thoughts are experienced as intrusive and unwanted, whether compulsions or rituals are present, and what the person believes will happen if they do not respond to the thought.
A small comparison table helps because it forces the decision into the open:
| Question | Disorder A | Disorder B |
| — | — | — |
| What is shared? | Similar symptom | Similar symptom |
| What separates them? | Decision point | Decision point |
| What mistake is easy? | Overweight one symptom | Ignore the pattern |
Practical takeaway: do not ask only “what symptoms are present?” Ask “which feature changes the diagnosis?” That is where differential diagnosis becomes clearer.
Study specifiers as meaning, not decoration
Specifiers often get treated as extra material, the part you will come back to later if there is time. That habit makes sense when you are overwhelmed, but it quietly weakens your clinical thinking. Specifiers are not decoration. They change how you describe the presentation.
A useful way to study a specifier is to ask what it adds:
- Does it change risk?
- Does it describe course?
- Does it clarify severity?
- Does it change what you would watch for clinically?
- Does it prevent a vague diagnosis?
That last question matters. A diagnosis without meaningful specifiers can hide clinically important information.
Mini case: a client meets criteria for major depressive disorder, but during the same episode they also report agitation, racing thoughts, decreased need for sleep, and increased goal-directed activity. If you treat specifiers as trivia, you may ignore the mixed-features question. If you understand why specifiers exist, you slow down and consider what that pattern means for formulation, risk, and supervision.
Common mistake: you memorize the names of specifiers without asking why they matter. What works better is to attach each specifier to a clinical purpose. Anxious distress, mixed features, melancholic features, psychotic features, peripartum onset, and seasonal pattern are not just labels. They tell you what kind of presentation you are looking at.
Use short cases to test whether you actually understand
You do not know a DSM-5-TR concept well until you can use it with a case. This is where the difference between recognition and recall becomes uncomfortable. A criterion can look familiar on the page and still disappear the moment you need to apply it. Recognition is not the same thing as recall.
Create short cases for yourself. Keep them simple: age, presenting problem, duration, impairment, and one complicating detail. Then ask what diagnosis you are considering, what evidence supports it, what evidence is missing, and what else you would need to rule out.
Example: a graduate student reports two months of low mood, loss of interest, early morning waking, guilt, low energy, and poor concentration. They also mention a four-day period last year when they slept three hours a night, felt unusually confident, talked more than usual, and started several projects, without marked impairment. That detail should interrupt your first impression. You are not only thinking about major depressive disorder anymore. You need to ask about hypomanic history and bipolar II disorder.
What usually goes wrong is that you decide too soon. You see enough symptoms to support one diagnosis and stop looking for the detail that could change it. What works better is to practice saying: “What finding would make me change my mind?” That question trains diagnostic humility without making you indecisive.
Watch for the mistakes that make DSM-5-TR study feel harder
Several mistakes make DSM study feel harder than it has to be. The first is studying disorders as isolated islands. You learn one set of criteria today and another tomorrow, but real vignettes test the space between them. If you do not study overlap, ordinary diagnostic ambiguity feels like a trick.
The second mistake is treating every detail as equally important. Some details are threshold decisions. Some are descriptive. Some are specifiers. Some are rule-outs. If you put them in the same mental bucket, you create unnecessary load. Not every detail has the same diagnostic weight.
The third mistake is mistaking familiar wording for usable knowledge. You may recognize a criterion because you have read it five times. That does not mean you can use it in a case. To test yourself, close the manual and write the criterion in your own words, then write one sentence about what evidence would support it.
Practical scenario: if you are considering PTSD, do not stop at “trauma plus distress.” Ask about the trauma exposure, intrusive symptoms, avoidance, negative mood and cognition changes, arousal, duration, impairment, and rule-outs. The goal is not to make the diagnosis feel mechanical. The goal is to know which pieces must be present before the label is justified.
What works better: after each disorder, write one line for each of these prompts: core pattern, useful feature, common confusion, rule-out, and one case detail that would change your mind. This is a small habit, but it builds the kind of structure that passive reading never gives you.
Review without rereading everything
Rereading feels productive because it is comfortable. The page is familiar, and familiar material gives you the feeling that you know it. But exams, supervision, and clinical conversations rarely ask you to recognize a paragraph. They ask you to retrieve, compare, justify, and apply.
A stronger review session starts with a blank page. Write the disorder family at the top. Without looking, list the disorders you remember, the core pattern for each one, the key time rules, and the main comparisons. Then open the DSM-5-TR and check what you missed. The gap tells you what to study next.
Practical takeaway: use “why not” questions. If you think a vignette fits major depressive disorder, ask why it is not bipolar II disorder, persistent depressive disorder, substance-induced depressive disorder, adjustment disorder, or grief. You do not need to force every case into every comparison, but the habit trains you to look for separating evidence.
Example exercise: after studying panic disorder, write three short cases. One should fit panic disorder, one should fit social anxiety disorder with panic attacks, and one should fit a substance-related panic presentation. Then compare them. That exercise teaches more than another hour of highlighting because it makes the diagnostic decision visible.
Common mistake: you review what already feels familiar because it is less uncomfortable. What works better is to review where retrieval breaks. If you cannot produce the core pattern from memory, that is the study target. If you cannot separate two similar disorders, that comparison belongs in your next session.
Create a weekly study routine you can repeat
A good DSM-5-TR study routine is boring in the best way. It should be simple enough that you can repeat it when the semester gets busy, supervision feels demanding, or exam pressure starts to build. The goal is not one heroic weekend with the manual. The goal is repeated practice with structure, comparison, recall, and application.
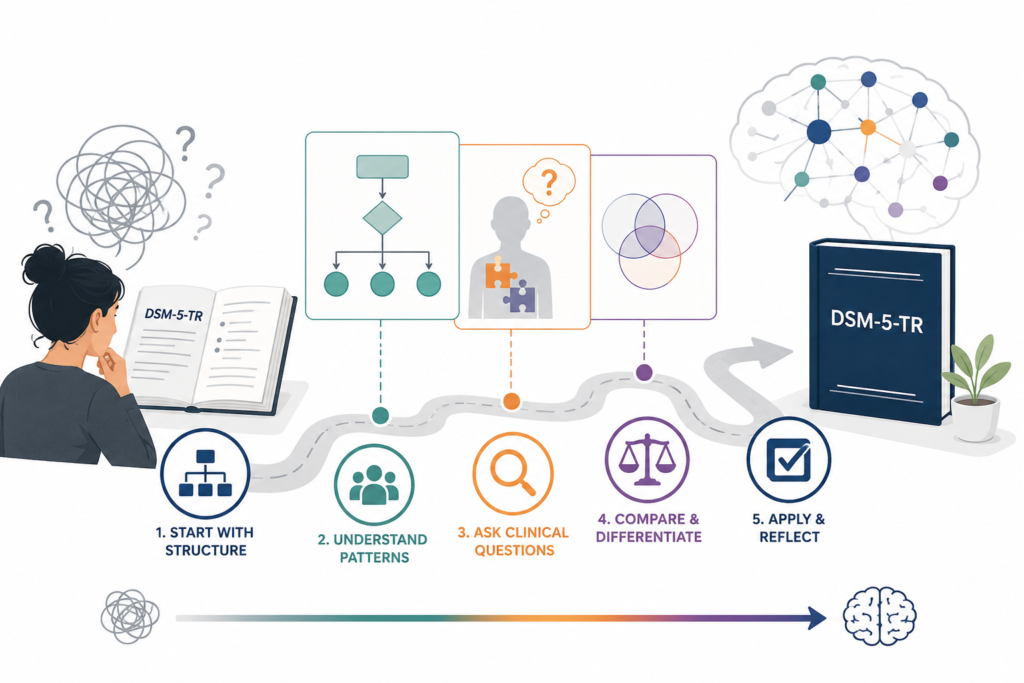
Try this weekly rhythm:
- Day 1: build the disorder-family map.
- Day 2: compare two similar disorders.
- Day 3: turn criteria into assessment questions.
- Day 4: test yourself with short cases.
- Day 5: review specifiers, rule-outs, and mistakes.
This routine works because it makes you do the things DSM study actually requires. You organize, retrieve, compare, and apply.
If you only have thirty minutes, use a smaller version: ten minutes for the map, ten minutes for one case, and ten minutes for the mistake you made. That final step matters. Your confusion is not a sign that you failed. It is a pointer. It tells you where your next study session should go.
Scenario: you keep confusing bipolar II disorder with major depressive disorder. Do not reread both sections from the beginning. Build a comparison around hypomanic history, episode pattern, impairment, and what the vignette does or does not say. Then write one mini case for each. You will feel the distinction much more clearly because you have practiced the decision, not just the wording.
Over time, this changes your relationship with the manual. The DSM-5-TR stops looking like an enormous wall of text and starts becoming a set of clinical decision tools. You still need supervision, humility, and careful context. But you are no longer treating every line as equally important. You are learning where to look, what to ask, and how to think.
Study resource: DSM-5-TR Visual Reference Guide
If your main problem is not motivation but organization, the DSM-5-TR Visual Reference Guide can be useful as a visual companion to your DSM-5-TR study routine.
Use it as a way to organize diagnostic patterns, compare overlapping disorders, and reduce cognitive load while you practice clinical reasoning. It should not replace the DSM-5-TR, coursework, supervision, or careful case formulation.
The best use is simple: study the manual, build your diagnostic map, then use the guide to check whether you understand the pattern behind the criteria rather than only recognizing the wording.
What to do next
Choose one disorder family and build a one-page map before you read another chapter. Add the core pattern, time rule, impairment rule, main rule-outs, and two close comparisons. Then test yourself with one short case. If you can explain why the diagnosis fits and what else you would need to rule out, you are studying the DSM-5-TR in a way that will actually carry into exams, supervision, and clinical work.